
Puncture Zone concept - Attempt at ideal puncture tech
- Jun 9, 2025
- 2 min read
An ideal percutaneous renal access has been defined as a single possible straight line along the calyceal axis. This can only be one possible line and achieved only with Bull’s eye technique for a given calyx by keeping the calyx along with its infundibular axis as a bull’s eye with the C-arm fluoroscopy. Here the C-arm axis, point of puncture on skin as well as the direction of entry get decided by themselves with the surgeon playing no role. However, most-surgeons try to describe their own techniques by doing Bull’s eye technique in 0, 30, cranial/caudal or any other random tilt of C-arm achieving decent puncture, good stone free rates and minimal complications. The literature is flooded with different techniques of PCNL puncture with different names. We understand the PCNL puncture concept as an Ideal puncture Zone, not limiting the ideal concept as a single tract. This has been published and is available for review.
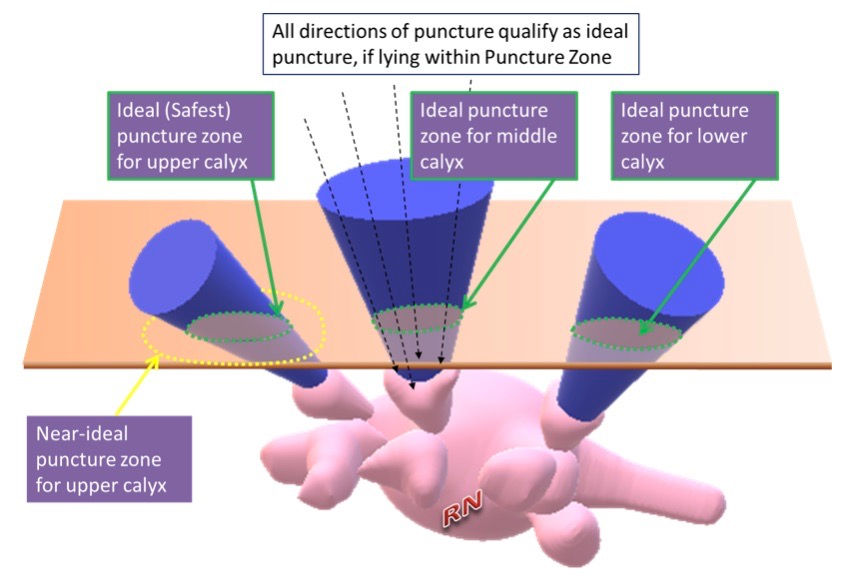
This concept (Figure 1) emphasizes that there is a large ideal ‘Puncture Zone’ as against any single ideal ‘Puncture Tract’ for any calyceal entry. It continues to encompass all properties of an ideal access tract. The largest imaginary cone that can fit into a respective calyx, with its tip in the pelvis defines the ‘Puncture zone’ for that calyx. A puncture done through any point on the base of this ‘Puncture Zone’ would fall into the category of an ideal ‘Puncture Tract’ for that calyx, indicating that geometrically there can be many ideal puncture tracts for entry into any particular calyx.
By understanding this concept, one can easily reconcile why so many different type of puncture techniques, from different points on skin, in different C-arm alignments, with Bull’s eye or Triangulation techniques, all still end up providing reasonable access for stone clearance. This ideal puncture zone can also be marked during actual PCNL cases by marking four points on the skin corresponding to the edges of the chosen infundibulum using C-arm. The tip of a needle is kept on the skin and a Bull’s eye is made with edge of infundibulum keeping C-arm in cranial tilt for identifying cranial-most point. Over- or undertilting of C-arm is avoided by carefully looking at fluoroscopy image so that the length of infundibulum just remains indiscernible and is visible only as a tangential. The same procedure is repeated in 4 different planes. After marking cranial-most point, the caudal-most edge of calyx is marked with C-arm in caudal tilt; lateral-most point is marked in lateral tilt and medial-most point is marked in medial tilt. These 4 surface markings can then be joined together in a curvilinear fashion to mark the ideal puncture zone specific for that calyx. Actual puncture site and alignment within this zone is then tailored as per individual patient’s renal or stone anatomy, and safety of surrounding structures.
Not only Ideal puncture zone, there is further surrounding area of near-ideal zone, which may also be reasonable enough in a large proportion of cases. As long as entry point is at the forniceal cup-end and not in the infundibulum-direct, one may get away without much complications.
by Dr Rishi Nayyar, AIIMS, New Delhi


Comments